Healing of rickets was assessed at week 40 in pediatric patients.
Meet Cora,real CRYSVITA patient
Meet Cora,a real CRYSVITA patient
CRYSVITA was effective in treating XLH1
A phase 3 study showed that CRYSVITA:1
Helped heal rickets and reduce rickets severity
Increased growth
Increased and sustained serum phosphorus levels
Study Design
Study 1 | Phase 3, randomized1
CRYSVITA was studied in a 64-week randomized, open-label phase 3 study (Study 1) in 61 children with XLH between 1 and 12 years of age. Study 1 compared treatment with CRYSVITA (n=29) every 2 weeks to conventional therapy (n=32) that included oral phosphate and active vitamin D supplements. Patients randomized to CRYSVITA received a mean dose of approximately 0.90 mg/kg (range 0.8-1.2 mg/kg) every 2 weeks.1
Group A
Crysvita
Mean dose of 0.90 mg/kg (range 0.8-1.2 mg/kg) every 2 weeks (n=29)
Group B
Conventional therapy
(Oral phosphate + vitamin D supplements) every 2 weeks (n=32)
Weeks 0-64
Open-label treatment period
Primary endpoint:2
Healing of rickets at week 40, as assessed by Radiographic Global Impression of Change (RGI-C) scores
Secondary endpoints:3
Lower extremity skeletal abnormalities, as assessed by the RGI-C long leg score
Severity of rickets, as measured by total Thacher Rickets Severity Score (RSS)
Growth, as measured by standing height z-score
Fasting serum phosphorus levels
Alkaline phosphatase (ALP) activity
Assessment of RGI-C at week 64
Proportion of patients with mean RGI-C score 2.0
Safety endpoint:3
Number of patients with adverse events (AEs), serious adverse events (SAEs), and AEs leading to discontinuation
Disease burden at baseline1,3
Category
Study 1 (n=61)
Mean age, years (range)
6.3 (1-12)
Male, n (%)
27 (44%)
Mean serum phosphorus (SD)
2.4 (0.26) mg/dL
Radiographic evidence of rickets, %
100%
Prior therapy, including oral phosphate and active vitamin D analogs, %
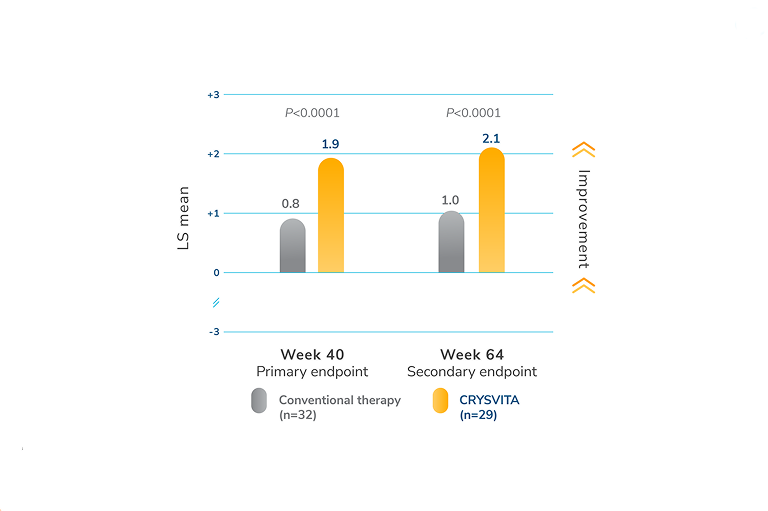
LS mean (95% CI) RGI-C score in patients treated with CRYSVITA was +1.9 (+1.70, +2.14), indicating that healing of rickets occurred, compared with +0.8 (+0.56, +0.99) in the conventional therapy group
Week 64 (primary endpoint):1
Findings from week 40 were maintained at week 64 (LS mean [95% CI] RGI-C global score at week 64 was +2.1 (+1.91, +2.20) for CRYSVITA group and +1.0 (+0.77, +1.30) for conventional therapy group)
* RGI-C at week 40 was the primary endpoint of the study. The estimates of LS mean for week 40 are from an ANCOVA model accounting for treatment group, baseline RSS, and baseline age stratification factor. The estimates for week 64 are from a GEE model accounting for treatment group, visit, treatment-by-visit interaction, baseline RSS, and baseline age stratification factor. Two-sided 95% CIs were utilized. The P-values were reported as nominal. No adjustment on multiplicity was made.1,2
ANCOVA=analysis of covariance; CI=confidence interval; GEE=generalized estimation equation; LS=least squares; RGI-C=Radiographic Global Impression of Change; RSS=Thacher Rickets Severity Score; SE=standard error.
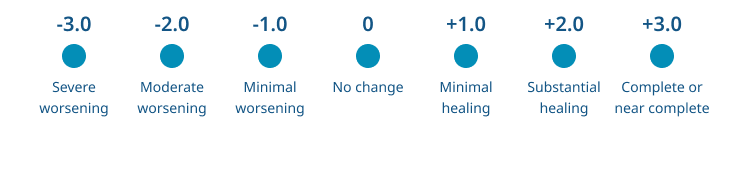
The Radiographic Global Impression of Change (RGI-C)
RGI-C is a 7-point scoring method (-3=severe worsening; 0=no change; +3=near/complete healing).1,2,5
RGI-C scores assess changes in the severity of rickets using the disease-specific qualitative RGI-C scoring system5,6
RGI-C scores are assigned by 3 independent experts blinded to treatment and patient2
An RGI-C score of +2.0 indicates substantial healing of rickets1
A figure showing the Radiographic Global Impression of Change scoring scale
-3.0 – Severe worsening
-2.0 – Moderate worsening
-1.0 – Minimal worsening
0 – No change
+1.0 – Minimal healing
+2.0 – Substantial healing
+3.0 – Complete or near complete
Secondary endpoint
CRYSVITA helped more patients achieve substantial healing of rickets compared with conventional therapy2
72%
of patients receiving CRYSVITA achieved substantial healing† of rickets2
P0.0001†
6%
of patients receiving conventional therapy2
At week 40, more patients receiving CRYSVITA achieved substantial healing of rickets (RGI-C score of ≥+2.0) compared with patients receiving conventional therapy (P<0.0001):2,†
CRYSVITA arm: 72% (21 out of 29)
Conventional therapy arm: 6% (2 out of 32)
These results were maintained at week 64.2
†An RGI-C score of +2.0 indicates a substantial healing of rickets. Proportion of patients with mean RGI-C score ≥+2.0 was a secondary endpoint of the study. Two-sided P-value was based on a logistic regression model, which included treatment group and baseline age stratification factor as independent variables and baseline RSS score as a continuous covariate. The P-value was reported as nominal. No adjustment on multiplicity was made.2
RGI-C=Radiographic Global Impression of Change; RSS=Thacher Rickets Severity Score.
The Radiographic Global Impression of Change (RGI-C)
RGI-C is a 7-point scoring method (-3=severe worsening; 0=no change; +3=near/complete healing).1,2,5
RGI-C scores assess changes in the severity of rickets using the disease-specific qualitative RGI-C scoring system5,6
RGI-C scores are assigned by 3 independent experts blinded to treatment and patient2
An RGI-C score of +2.0 indicates substantial healing of rickets1
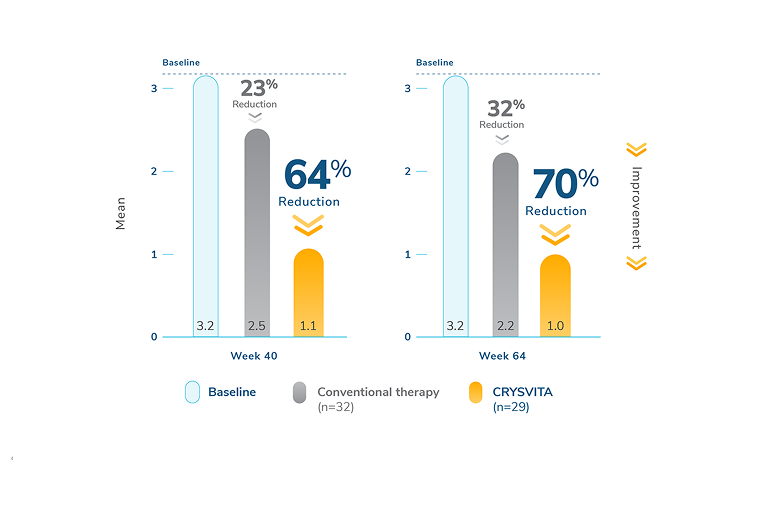
Treatment every 2 weeks with CRYSVITA showed a reduction in mean total rickets severity, compared with conventional therapy, as assessed using the Thacher Rickets Severity Score (RSS). A reduced RSS score indicates improvement in rickets severity.1
‡The estimates of LS mean for week 40 are from an ANCOVA model accounting for treatment group, baseline RSS, and baseline age stratification factor. The estimates for week 64 are from a GEE model accounting for treatment group, visit, treatment-by-visit interaction, baseline RSS, and baseline age stratification factor.1
RSS is a 10-point score for radiographs of wrists and knees to assess the degree of metaphyseal fraying and cupping and the proportion of the growth plate affected.1,2,7
It is a predefined scale that evaluates specific abnormalities in the wrists and knees1,2,7
Total points progress in half-point increments from 0-10: wrists (0-4) plus knees (0-6)
RSS is assigned by an independent expert blinded to treatment, treatment duration, and radiographic sequence2,7
Higher scores indicate a more severe state of rickets, and a reduction in RSS indicates an improvement in severity1,2,7
X-ray images of two pairs of legs with skeletal abnormalities at baseline and after 64 weeks of treatment with CRYSVITA or conventional therapy.
Individual results may vary.
At week 64, CRYSVITA maintained greater improvement in lower extremity skeletal abnormalities compared with conventional therapy, as assessed by RGI-C (LS mean [SE]: +1.25 [0.17] vs +0.29 [0.12]).1,§
The radiographic examples show the following:1,4
A patient with XLH (female, 2.9 years of age) who received CRYSVITA every 2 weeks for 64 weeks
A patient (also female, 2.9 years of age) who continued on conventional therapy
§The estimates for week 64 are from a GEE model accounting for treatment group, visit, treatment-by-visit interaction, baseline RSS, and baseline age stratification factor.1
GEE=generalized estimation equation; LS=least squares; RGI-C=Radiographic Global Impression of Change; RSS=Thacher Rickets Severity Score; SE=standard error.
Growth increase
Secondary endpoint
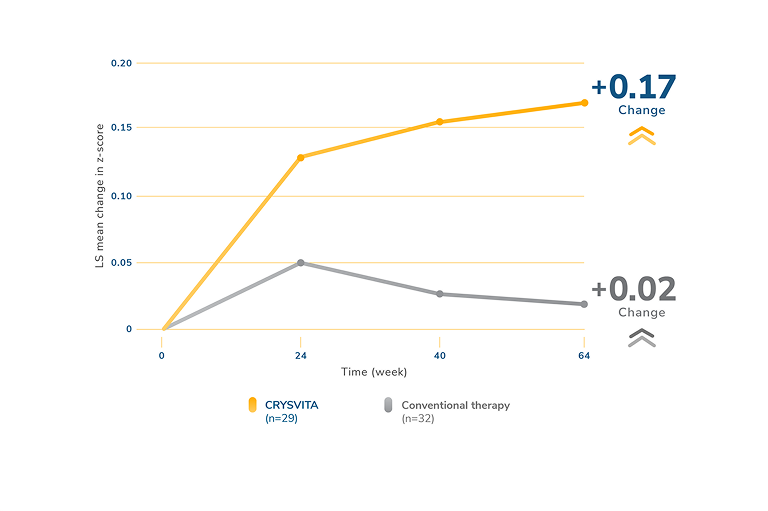
CRYSVITA increased growth compared to conventional therapy1,2
Height z-scores with CRYSVITA every 2 weeks vs conventional therapy2,||
At 64 weeks, the following improvements were seen in standing mean (SD) height z-score:1
In patients who received CRYSVITA every 2 weeks: z-score increased from -2.32 (1.17) at baseline to -2.11 (1.11)
In patients who received conventional therapy: z-score increased from -2.05 (0.87) at baseline to -2.03 (0.83)
||The estimates of LS mean and SE are from a GEE model, which included change from baseline for recumbent length/standing height z-score as the dependent variable, treatment group, visit, interaction between treatment group by visit, and baseline RSS stratification as factors; and age and baseline recumbent length/standing height z-score as continuous covariates, with exchangeable covariance structure.2
The standing height z-score was used as a measurement for growth
The “stature-for-age” z-score was determined based on a percentile basis using the Centers for Disease Control and Prevention/National Center for Health Statistics (CDC/NCHS) Clinical Growth Charts
Standing height was used to calculate the stature-for-age z-score based on standardized age- and sex-adjusted stature from the CDC
Change in serum phosphorus levels
Secondary endpoint
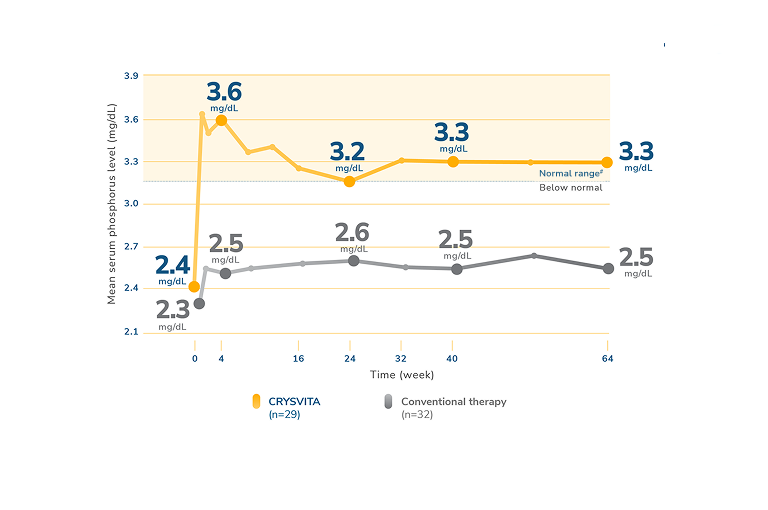
CRYSVITA increased and maintained serum phosphorus levels1
Mean serum phosphorus levels in children receiving CRYSVITA or conventional therapy1,¶
In Study 1, CRYSVITA increased mean (SD) serum phosphorus levels from 2.4 (0.24) mg/dL at baseline to 3.3 (0.43) mg/dL at week 40 and to 3.3 (0.42) mg/dL at week 64. In the conventional therapy group, mean (SD) serum phosphorus concentrations increased from 2.3 (0.26) mg/dL at baseline to 2.5 (0.34) mg/dL at week 40 and to 2.5 (0.39) mg/dL at week 64.1
An increase in serum phosphorus levels compared with conventional therapy was observed with CRYSVITA at week 1 and maintained through week 64.1,3
Serum alkaline phosphatase activity:
For Study 1, mean (SD) total serum alkaline phosphatase activity decreased from 511 (125) U/L at baseline to 337 (86) U/L in the CRYSVITA group (mean change: -33%) and from 523 (154) U/L at baseline to 495 (182) U/L in the conventional therapy group (mean change: -5%) at week 64.1
¶Mean serum phosphorus level (mg/dL). Lower limit of normal (LLN) is 3.2 mg/dL.1
#Normal levels of serum phosphorus range from 3.2 mg/dL to 6.1 mg/dL. Note that the normal levels of serum phosphorus vary by age and sex.3,8
SD=standard deviation.
Safety
Safety endpoint
CRYSVITA clinical safety profile in children with XLH
Most common adverse reactions (≥10%) in patients treated with CRYSVITA observed in Study 11,**
n=total number of patients who received at least 1 dose of CRYSVITA or conventional therapy.
**≥10% in the CRYSVITA group that also occurred at a higher frequency than the conventional therapy group.1
††Injection site reaction includes: injection site reaction, injection site erythema, injection site pruritus, injection site swelling, injection site pain, injection site rash, injection site bruising, injection site discoloration, injection site discomfort, injection site hematoma, injection site hemorrhage, injection site induration, injection site macule, and injection site urticaria.1,
‡‡Cough includes: cough and productive cough.1,
§§Tooth abscess includes: tooth abscess, tooth infection, and toothache.1,
||||Vitamin D decreased includes: vitamin D deficiency, blood 25-hydroxycholecalciferol decreased, and vitamin D decreased.1,
The most frequent hypersensitivity reactions in the CRYSVITA arm were rash (10%), injection site rash (10%), and injection site urticaria (7%).1
Hyperphosphatemia
In pediatric studies, there were no events of hyperphosphatemia reported.1
Injection site reaction
Fifty-two percent of patients in the CRYSVITA arm had a local injection site reaction (e.g., injection site urticaria, erythema, rash, swelling, bruising, pain, pruritus, and hematoma) at the site of injection. Injection site reactions were generally mild in severity, occurred within 1 day of injection, lasted approximately 1 to 3 days, required no treatment, and resolved in almost all instances.1
Immunogenicity
As with all therapeutic proteins, there is potential for immunogenicity. The detection of antibody formation is highly dependent on the sensitivity and specificity of the assay. Additionally, the observed incidence of antibody (including neutralizing antibody) positivity in an assay may be influenced by several factors, including assay methodology, sample handling, timing of sample collection, concomitant medications, and underlying disease. For these reasons, comparison of the incidence of antibodies to CRYSVITA in the studies described in this website with the incidence of antibodies in other studies or to other products may be misleading.1
In XLH clinical studies, none (0/13) of the 1- to 4-year-old patients, 19% (10/52) of the 5- to 12-year-old patients, and 15% (20/131) of the adult patients tested positive for anti-drug antibodies (ADA) after receiving CRYSVITA. Among these, three 5- to 12-year-old patients tested positive for neutralizing antibodies. The presence of ADA was not associated with clinically relevant changes in pharmacokinetics, pharmacodynamics, efficacy, and safety of burosumab in patients with XLH.1
Meet Cora,a real CRYSVITA patient
Want to learn more about starting your pediatric patients on CRYSVITA?
CRYSVITA® (burosumab-twza) is a fibroblast growth factor 23 (FGF23) blocking antibody indicated for the treatment of X-linked hypophosphatemia (XLH) in adult and pediatric patients 6 months of age and older.
Important Safety Information
CONTRAINDICATIONS
CRYSVITA is contraindicated:
In concomitant use with oral phosphate and/or active vitamin D analogs (e.g., calcitriol, paricalcitol, doxercalciferol, calcifediol) due to the risk of hyperphosphatemia.
When serum phosphorus is within or above the normal range for age.
In patients with severe renal impairment or end stage renal disease because these conditions are associated with abnormal mineral metabolism.
WARNINGS AND PRECAUTIONS
Hypersensitivity
Hypersensitivity reactions (e.g., rash, urticaria) have been reported in patients with CRYSVITA. Discontinue CRYSVITA if serious hypersensitivity reactions occur and initiate appropriate medical treatment.
Hyperphosphatemia and Risk of Nephrocalcinosis
Increases in serum phosphorus to above the upper limit of normal may be associated with an increased risk of nephrocalcinosis. For patients already taking CRYSVITA, dose interruption and/or dose reduction may be required based on a patient’s serum phosphorus levels.
Injection Site Reactions
Administration of CRYSVITA may result in local injection site reactions. Discontinue CRYSVITA if severe injection site reactions occur and administer appropriate medical treatment.
ADVERSE REACTIONS
Pediatric Patients
Adverse reactions reported in 10% or more of CRYSVITA-treated pediatric XLH patients across three studies are: pyrexia (55%, 44%, and 62%), injection site reaction (52%, 67%, and 23%), cough (52%), vomiting (41%, 48%, and 46%), pain in extremity (38%, 46%, and 23%), headache (34% and 73%), tooth abscess (34%, 15%, and 23%), dental caries (31%), diarrhea (24%), vitamin D decreased (24%, 37%, and 15%), toothache (23% and 15%), constipation (17%), myalgia (17%), rash (14% and 27%), dizziness (15%), and nausea (10%).
Adverse reactions reported in more than 5% of CRYSVITA-treated adult XLH patients and in at least 2 patients more than placebo in one study are: back pain (15%), headache (13%), tooth infection (13%), restless legs syndrome (12%), vitamin D decreased (12%), dizziness (10%), constipation (9%), muscle spasms (7%), and blood phosphorus increased (6%).
Spinal stenosis is prevalent in adults with XLH, and spinal cord compression has been reported. It is unknown if CRYSVITA therapy exacerbates spinal stenosis or spinal cord compression.
USE IN SPECIFIC POPULATIONS
There are no available data on CRYSVITA use in pregnant women to inform a drug-associated risk of adverse developmental outcomes. Serum phosphorus levels should be monitored throughout pregnancy. Report pregnancies to the Kyowa Kirin, Inc. Adverse Event reporting line at 1-844-768-3544.
There is no information regarding the presence of CRYSVITA in human milk or the effects of CRYSVITA on milk production or the breastfed infant. Therefore, the developmental and health benefits of breastfeeding should be considered along with the mother’s clinical need for CRYSVITA and any potential adverse effects on the breastfed infant from CRYSVITA or from the underlying maternal condition.
PATIENT COUNSELLING INFORMATION
Advise patients not to use any oral phosphate and/or active vitamin D analog products.
Instruct patients to contact their physician if hypersensitivity reactions, injection site reactions, and restless legs syndrome induction or worsening of symptoms occur.
You may report side effects to the FDA at (800) FDA-1088 or www.fda.gov/medwatch.
You may also report side effects to Kyowa Kirin, Inc. at 1-844-768-3544.
For important risk and use information, please see the full Prescribing Information for CRYSVITA.
Indication
CRYSVITA® (burosumab-twza) is a fibroblast growth factor 23 (FGF23) blocking antibody indicated for the treatment of X-linked hypophosphatemia (XLH) in adult and pediatric patients 6 months of age and older.
Important Safety Information
CONTRAINDICATIONS
CRYSVITA is contraindicated:
In concomitant use with oral phosphate and/or active vitamin D analogs (e.g., calcitriol, paricalcitol, doxercalciferol, calcifediol) due to the risk of hyperphosphatemia.
When serum phosphorus is within or above the normal range for age.
In patients with severe renal impairment or end stage renal disease because these conditions are associated with abnormal mineral metabolism.
WARNINGS AND PRECAUTIONS
Hypersensitivity
Hypersensitivity reactions (e.g., rash, urticaria) have been reported in patients with CRYSVITA. Discontinue CRYSVITA if serious hypersensitivity reactions occur and initiate appropriate medical treatment.
Hyperphosphatemia and Risk of Nephrocalcinosis
Increases in serum phosphorus to above the upper limit of normal may be associated with an increased risk of nephrocalcinosis. For patients already taking CRYSVITA, dose interruption and/or dose reduction may be required based on a patient’s serum phosphorus levels.
Injection Site Reactions
Administration of CRYSVITA may result in local injection site reactions. Discontinue CRYSVITA if severe injection site reactions occur and administer appropriate medical treatment.
ADVERSE REACTIONS
Pediatric Patients
Adverse reactions reported in 10% or more of CRYSVITA-treated pediatric XLH patients across three studies are: pyrexia (55%, 44%, and 62%), injection site reaction (52%, 67%, and 23%), cough (52%), vomiting (41%, 48%, and 46%), pain in extremity (38%, 46%, and 23%), headache (34% and 73%), tooth abscess (34%, 15%, and 23%), dental caries (31%), diarrhea (24%), vitamin D decreased (24%, 37%, and 15%), toothache (23% and 15%), constipation (17%), myalgia (17%), rash (14% and 27%), dizziness (15%), and nausea (10%).
Adverse reactions reported in more than 5% of CRYSVITA-treated adult XLH patients and in at least 2 patients more than placebo in one study are: back pain (15%), headache (13%), tooth infection (13%), restless legs syndrome (12%), vitamin D decreased (12%), dizziness (10%), constipation (9%), muscle spasms (7%), and blood phosphorus increased (6%).
Spinal stenosis is prevalent in adults with XLH, and spinal cord compression has been reported. It is unknown if CRYSVITA therapy exacerbates spinal stenosis or spinal cord compression.
USE IN SPECIFIC POPULATIONS
There are no available data on CRYSVITA use in pregnant women to inform a drug-associated risk of adverse developmental outcomes. Serum phosphorus levels should be monitored throughout pregnancy. Report pregnancies to the Kyowa Kirin, Inc. Adverse Event reporting line at 1-844-768-3544.
There is no information regarding the presence of CRYSVITA in human milk or the effects of CRYSVITA on milk production or the breastfed infant. Therefore, the developmental and health benefits of breastfeeding should be considered along with the mother’s clinical need for CRYSVITA and any potential adverse effects on the breastfed infant from CRYSVITA or from the underlying maternal condition.
PATIENT COUNSELLING INFORMATION
Advise patients not to use any oral phosphate and/or active vitamin D analog products.
Instruct patients to contact their physician if hypersensitivity reactions, injection site reactions, and restless legs syndrome induction or worsening of symptoms occur.
You may report side effects to the FDA at (800) FDA-1088 or www.fda.gov/medwatch.
You may also report side effects to Kyowa Kirin, Inc. at 1-844-768-3544.
For important risk and use information, please see the full Prescribing Information for CRYSVITA.
Reference:
1. CRYSVITA (burosumab-twza). US Prescribing Information. Kyowa Kirin, Inc. March 2023. 2. Imel EA, et al. Burosumab versus conventional therapy in children with X-linked hypophosphataemia: a randomised, active-controlled, open-label, phase 3 trial. Lancet. 2019;393(10189):2416-2427. 3. Data on file. 301 CSR. Ultragenyx Pharmaceutical Inc. 2018. 2022;17(1):30. 4. UX023-CL301 Picture Book. 2019. 5. Lim R, et al. Validation of the Radiographic Global Impression of Change (RGI-C) score to assess healing of rickets in pediatric X-linked hypophosphatemia (XLH). Bone. 2021;148:115964. 6. Whyte MP, et al. Validation of a Novel Scoring System for Changes in Skeletal Manifestations of Hypophosphatasia in Newborns, Infants, and Children: The Radiographic Global Impression of Change Scale. J Bone Miner Res. 2018;33(5):868-874. 7. Thacher TD, et al. Rickets severity predicts clinical outcomes in children with X-linked hypophosphatemia: Utility of the radiographic Rickets Severity Score. Bone. 2019;122:76-81. 8. Koek WNH, et al. Age-dependent sex differences in calcium and phosphate homeostasis. Endocr Connect. 2021;10(3):273-282.




 Show description
Show description